The Case Background
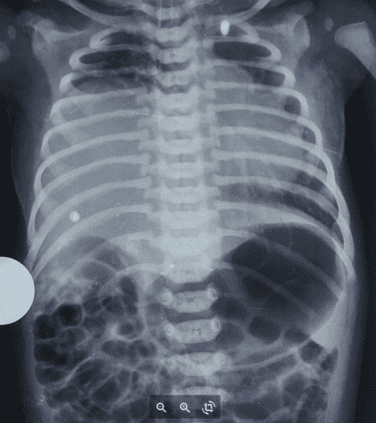
A term baby was admitted with respiratory distress. CXR revealed homogenous whiteout lungs bilaterally. The patient required immediate intubation, which was provided.
After the first dose of surfactant was given, the Fio2 requirement was gradually reduced. The second X-ray showed no changes in the widespread opacity of the lungs. Seeing no improvement, the baby was admitted to NICU Live.
Impact of NICU Live’s Intervention
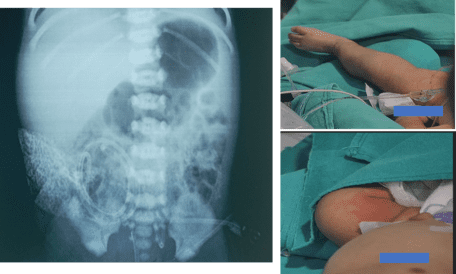
Urgent lung ultrasound was advised, to evaluate for pleural effusion, and it showed a large effusion. A pleural tap was done, followed by ICD placement. After these procedures, the next X-Ray taken showed well-expanded lungs, with improvement in the condition. The intubation was removed 48 hours later after doctors confirmed there was no accumulation of fluid in any other body spaces. The baby remained on IV antibiotics, and TPN, and was hemodynamically stable.
The assessments through NICU Live continued, and after initial stabilization, doctors recommended that feeds be gradually introduced with caution. However, In the next 12 hours, pleural fluid from ICD turned milky white, indicating chyle. Immediately, the enteral nutrition was stopped. A repeat pleural fluid analysis confirmed chylous effusion bilaterally. The baby was put on Octreotide infusion and it was graded up to achieve a response. After one week of medication, the chyle gradually started reducing. A surgical review was done, and we planned to do chemical pleurodesis if there was no response to octreotide. But the family wanted to take the discharge of the baby, against medical advice.
NICU Live Benefits
While congenital neonatal chylous pleural effusions are relatively rare and require clinical expertise and patience to diagnose and treat, they may turn dangerous if timely medical expert advice is not available. The intervention provided by NICU Live was priceless support to ensure a correct, timely diagnosis of the above case. It enabled the healthcare providers to administer the correct procedures and medication for the recovery of the newborn

 Toll Free Number
Toll Free Number